
Understanding Navicular Syndrome & Heel Pain in Horses
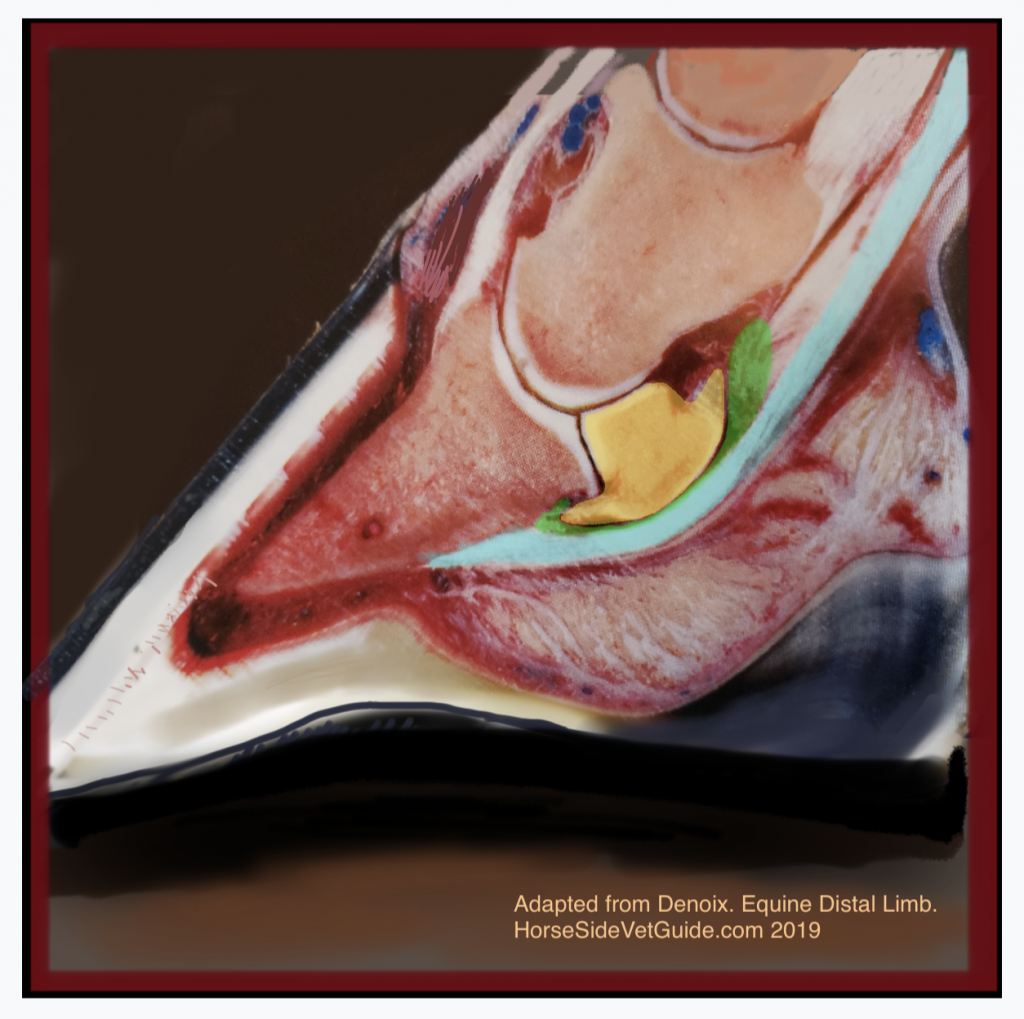
The cut section of a hoof, showing the important anatomy. Yellow- navicular bone, Green- navicular bursa, Turquoise- Deep Digital Flexor Tendon. The DDFT runs over bursa and bone and attaches on underside of P3. Image adapted from a photo in Denoix- The Distal Limb.
Navicular Syndrome (also called Podotrochleosis, Podotrochlitis, Palmar Foot Pain, Caudal Foot Pain,Heel Pain, and Chronic Heel Pain, among many others), typically involves degeneration of the navicular bone and the adjacent anatomy of the back half of the hoof, resulting in chronic lameness that usually involves both forefeet.
Conditions affecting the navicular bone and the surrounding structures are extremely important; they are estimated to make up fully one third of all chronic forelimb lameness in horses (Baxter 2011).
“NO FOOT – NO HORSE”
Maybe you have heard that old horseman’s saying. There is a lot of truth to it. The foundation of every horse is the foot.
In order to understand navicular syndrome, it’s necessary to understand the basic anatomy of the foot. The equine “foot” includes the hoof capsule and its associated structures, the lower end of the short pastern bone, the coffin bone (P3, Pedal bone) and the navicular bone. There is the “hoof complex” itself – the hoof capsule, sole, frog, digital cushion, and ungual (collateral) cartilages.
The coffin bone takes up approximately 2/3 of the hoof, and it is approximately the shape of the hoof. Running down the back of the limb, diving into the heel of the foot and attaching to the “palm” of the coffin bone, is a wide, flat very dense tendon called the deep digital flexor tendon (DDFT= turquoise on the image below). The action of the DDFT is to flex the coffin joint and provide the floor of the joint. It courses over the navicular bone, using it as a fulcrum near its attachment to the coffin bone.
Between the DDFT and the navicular bone is the navicular bursa, a “collapsed balloon” containing synovial fluid, which facilitates the sliding of the DDFT over the navicular bone. The navicular bone (named after its ship-like shape) sits wedged (as a fulcrum) deep to the DDFT, under the short pastern bone (P2) and behind the coffin bone, and redirects the force of the DDFT such that the mechanics work to counteract the tendency for the toe of the hoof to come off the ground in weight bearing. The navicular bone, therefore, is a vital, central part of the structure of the hoof. Because of the mechanics involved, the navicular bone is under tremendous compression with weight bearing. This area is unforgiving of trauma and of abnormal, excessive stress placed upon it.
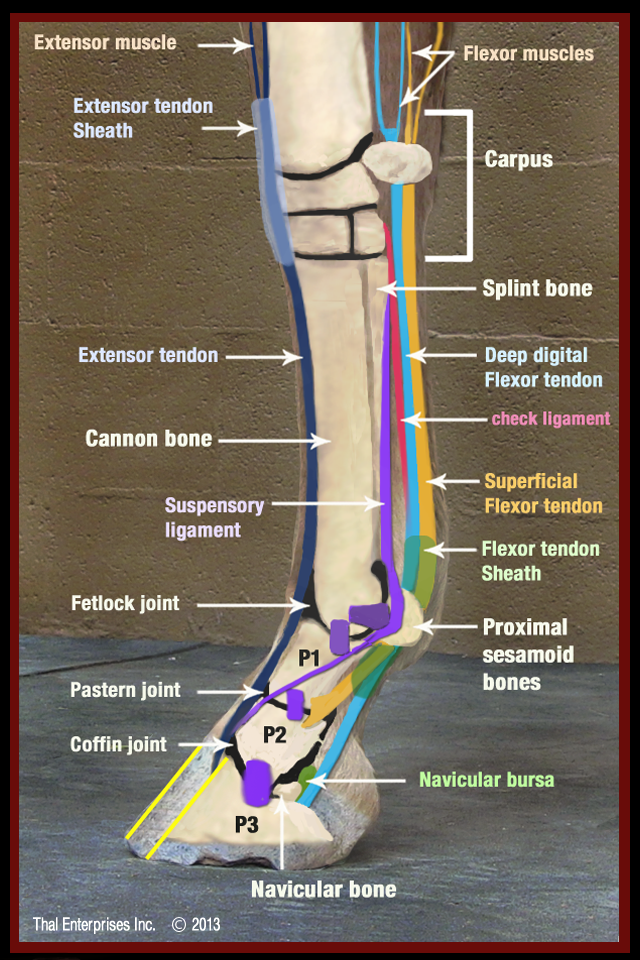
The major bone and soft tissue structures of the equine lower limb. Image courtesy HorseSideVetGuide.com
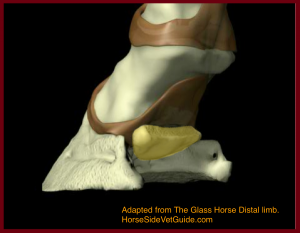
The navicular bone (yellow) shown with the hoof and soft tissues removed.
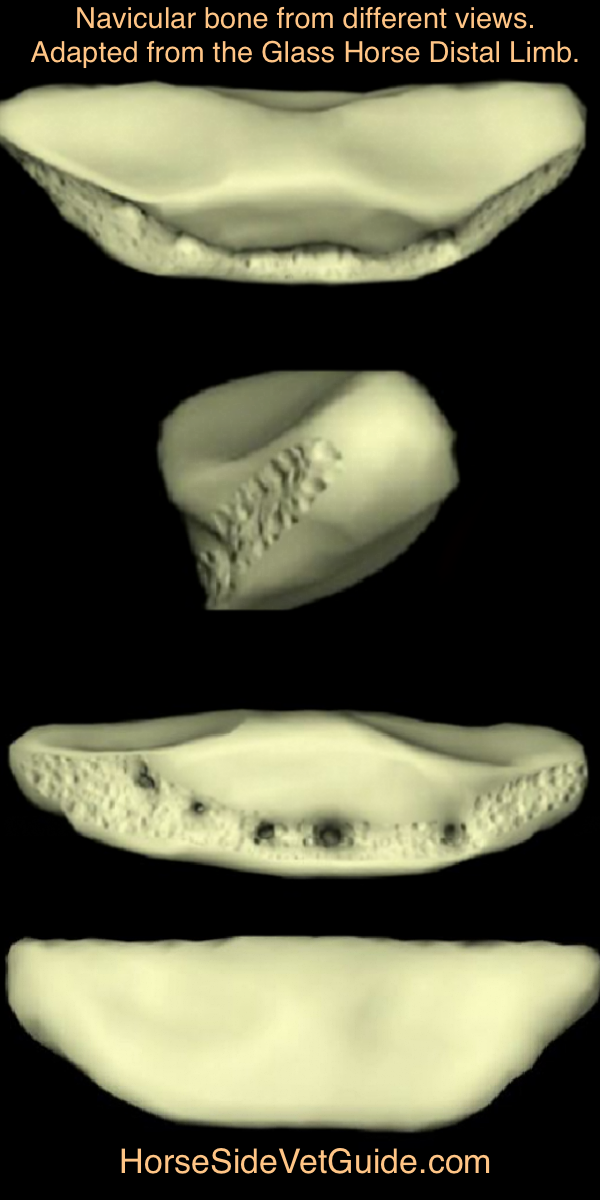
The navicular bone, as viewed from front, side, rear and from above.
Think of a standing horse, and imagine the fetlock (ankle) sagging down under the weight, into a sling created by the flexor tendons. The only flexor tendon that continues all the way into the hoof, to attach onto P3, is the deep digital flexor tendon (DDFT). With weight-bearing, the DDFT is stretched (under tension), from the horse’s weight and compresses the navicular bone under it.
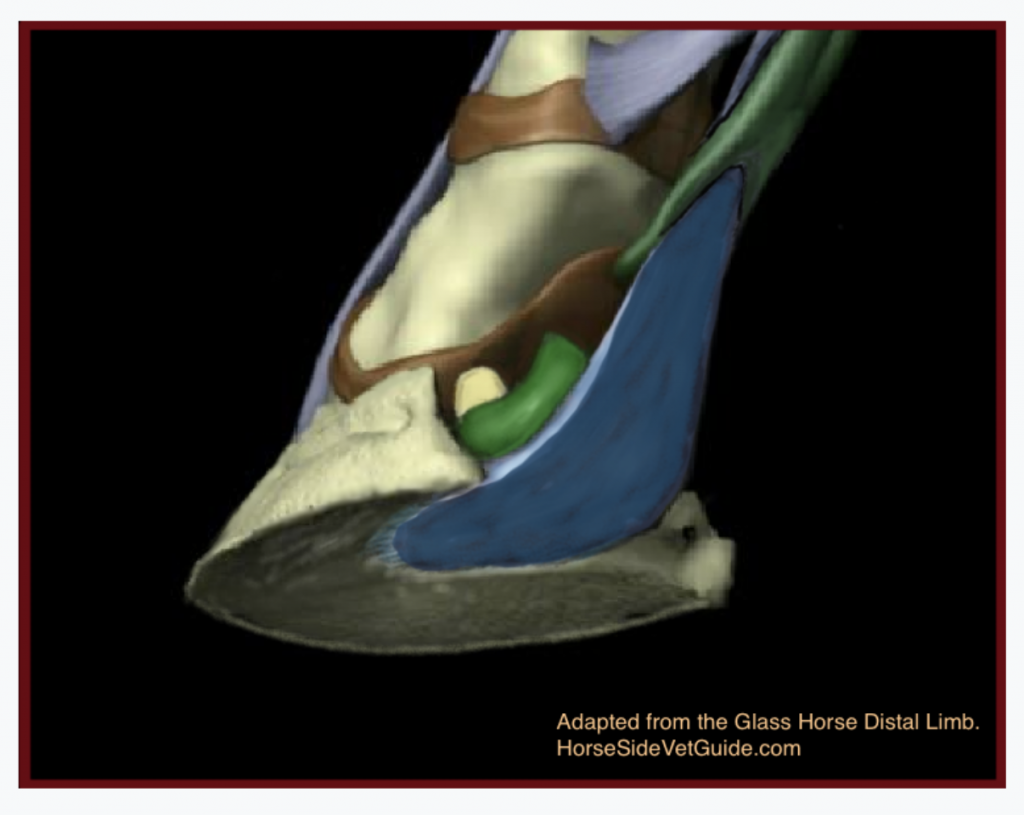
Looking from below, at the 7:00 position showing the DDFT (blue) attaching on P3 (Coffin bone), coursing over the bursa (green) and the navicular bone peeking out from behind (Yellow). Adapted from the Glass Horse Distal Limb.
The usual hallmark of navicular syndrome is some degeneration of the navicular bone. There are several theories about what starts this degenerative process. Excessive stress on the apparatus is likely to be a factor. We know that once damage occurs- similar to what happens in arthritis- a cycle begins wherein more inflammation causes more damage, leading to further inflammation and increasing lameness.
Changes to the bone include development of “holes” or cysts, damage to the cartilage on several of its surface, and damage to the supporting ligaments. The loss of smooth cartilage surface can lead to arthritis of the coffin joint, inflammation of the navicular bursa, and fraying of the DDFT, sometimes resulting in adhesion (“spot-welding” )of the DDFT to the navicular bone.
PREDISPOSING FACTORS
There are no hard and fast rules when it comes to predicting which horses will be affected by Navicular Syndrome, but there are some general trends:
.
- • Navicular Syndrome is most common in American Quarter Horses, but it also commonly affects Thoroughbreds and Warmblood breeds. It is rare in ponies and Arabians.
- • It most often affects horses with large, heavy bodies and small feet, but this is certainly not always the case.
- • While certain foot characteristics (long toe, low heel for example) are commonly associated with navicular syndrome, horses with feet of any size, shape or conformation can end up with the condition.
- • Unlike many arthritis-type lameness conditions, “classic” Navicular Syndrome/heel pain is most commonly seen in relatively young horses. The average age of onset is about 7 years.
- • We see cases in which poor shoeing or hoof care was likely to be a big factor. Other times, however, there is no such history.
- • We see horses in which there’s obviously a genetic or conformational predisposition.
- • A period of heavy use may seem to have triggered the process in some, but not all cases.
In many cases, we just don’t know how or why navicular problems start. Genetics, conformation, environment, hoof imbalance and poor shoeing, repetitive concussion and overload of the structures, and many other factors probably all come together to begin and perpetuate the process of Navicular Syndrome.
Over the last 15 years, the use of MRI to image the lower limbs of horses has shown us that lameness conditions in the heel of the foot are more complicated than we previously thought. MRI has revealed a host of soft tissue injury we could never before define.
WHAT YOU MIGHT OBSERVE – SIGNS OF NAVICULAR DISEASE
“My horse just seems stiff, or short. He’s not really lame, he’s just off…”
Navicular syndrome usually first appears as a very mild lameness that gradually worsens over weeks to months. It usually affects both front feet, but one often seems worse than the other. As with most lameness, the lameness from navicular syndrome is most noticeable at the trot, resulting in a head-bob. Affected horses often have a short, choppy trot and canter, and tend to hold their neck and poll rigid. The gradual onset of lameness in both forefeet can mislead riders into thinking that “this is just the way the horse travels”.
In subtle cases, all you may notice is that the horse may simply not perform to your expectations or will seem reluctant to work. The lameness or stiffness often will seem worse on hard ground, and might only be obvious in a small circle to one direction or another. When at rest, some affected horses will “point” the more painful foot (hold it out in front) to relieve pain in the heel.
Swelling, heat in the area, and digital pulse are generally subtle, or not present at all. Unlike the case with many injuries that result in lameness, lameness from navicular syndrome does not usually improve with rest.
DIAGNOSIS: THE VETERINARY LAMENESS EXAMINATION
Diagnosis of Navicular Syndrome is based on a thorough veterinary lameness exam that considers the horse’s type, breed, conformation, age, shoeing, and work and management history. Standing exam often shows predisposing conformation, but shows little inflammation or swelling anywhere in the limbs and variable responses to standing manipulation of the lower limbs. Horses that have heel pain will often (but not always) have distortions of the hoof capsule that provide clues- long toe, low heel, under-run or sheared heels (heels of uneven height).
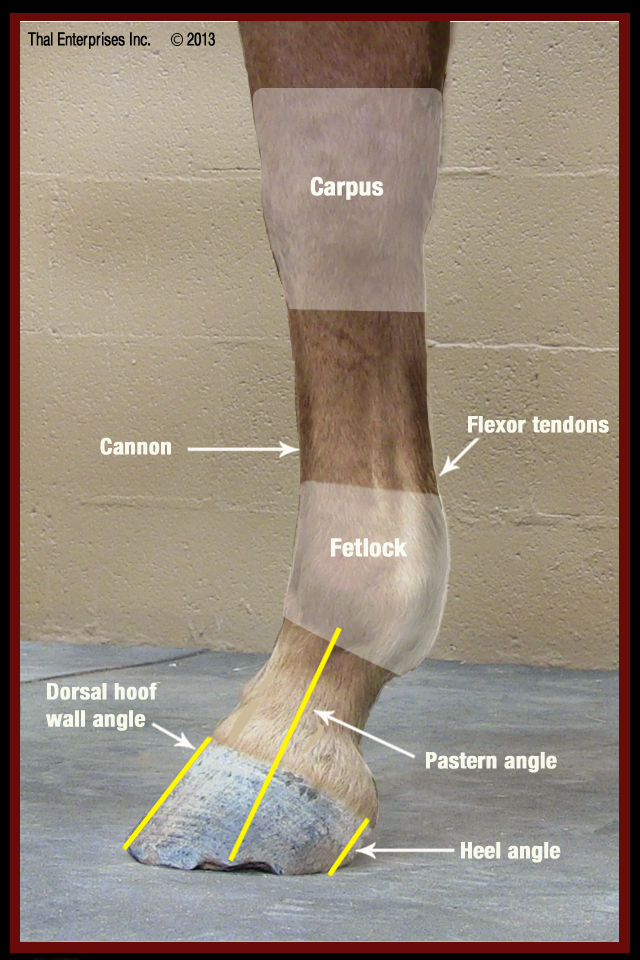
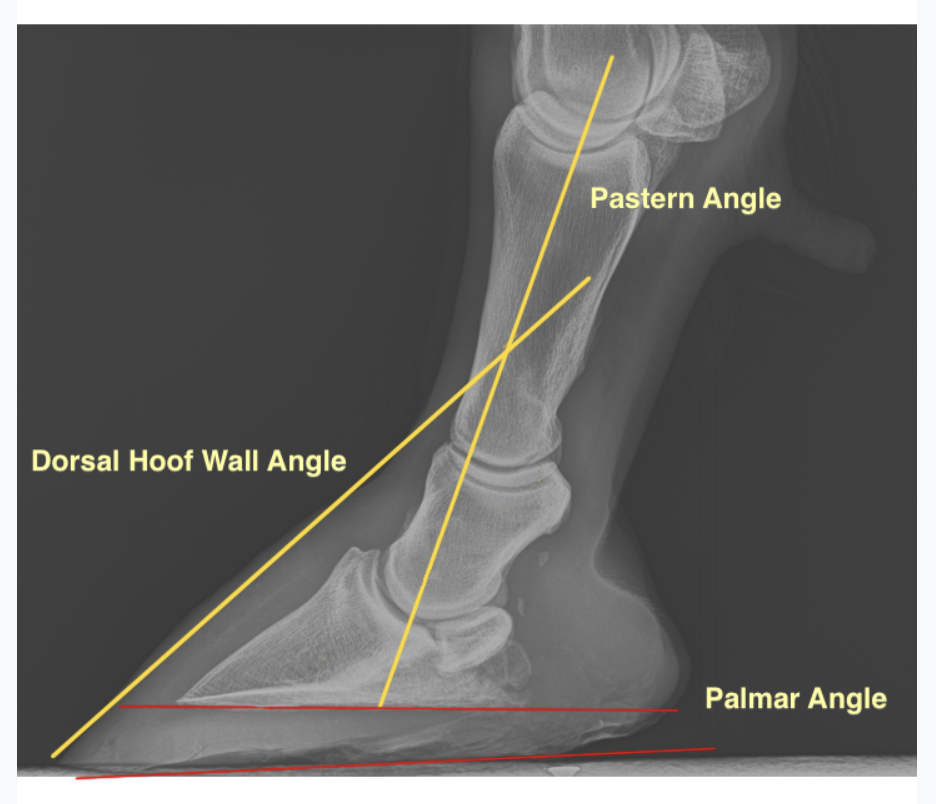
This illustrates pastern angle versus dorsal hoof wall angle. These two angles should be roughly similar. Many horses with Navicular Syndrome have lower hoof angle than pastern angle, but in some cases, the opposite. Image from HorseSideVetGuide.com
Observation of the horse at the trot usually shows lameness affecting both front limbs. In most cases, the lameness will be worse on the circle than on the straight, and worse on hard ground. Flexion exam responses are inconsistent. In many cases, hoof tester response is positive over the middle third of the frog, but this too is variable.

Viewing the front hooves from behind on a flat surface. This horse has inside and outside heels of each hoof that are roughly the same height, and the heel heights are also roughly same left to right. Image from HorseSideVetGuide.com
THE CORNERSTONE OF DIAGNOSIS – NERVE BLOCKS
A critical part of the exam to diagnose this condition is the use of diagnostic anesthesia (nerve blocks) in which the nerves that supply sensation to a region of the limb are temporarily anesthetized with a short-acting local anesthetic.
The common nerve block used for diagnosis of navicular syndrome is called the “palmar digital nerve block”(PDN). The PDNs are a pair of nerves that run along the rear of the pastern and supply sensation to not only the navicular bone, but also the sole, heel, frog, bars, digital cushion, deep flexor tendon in the hoof, supporting navicular ligaments and bursa, and some of the coffin joint.
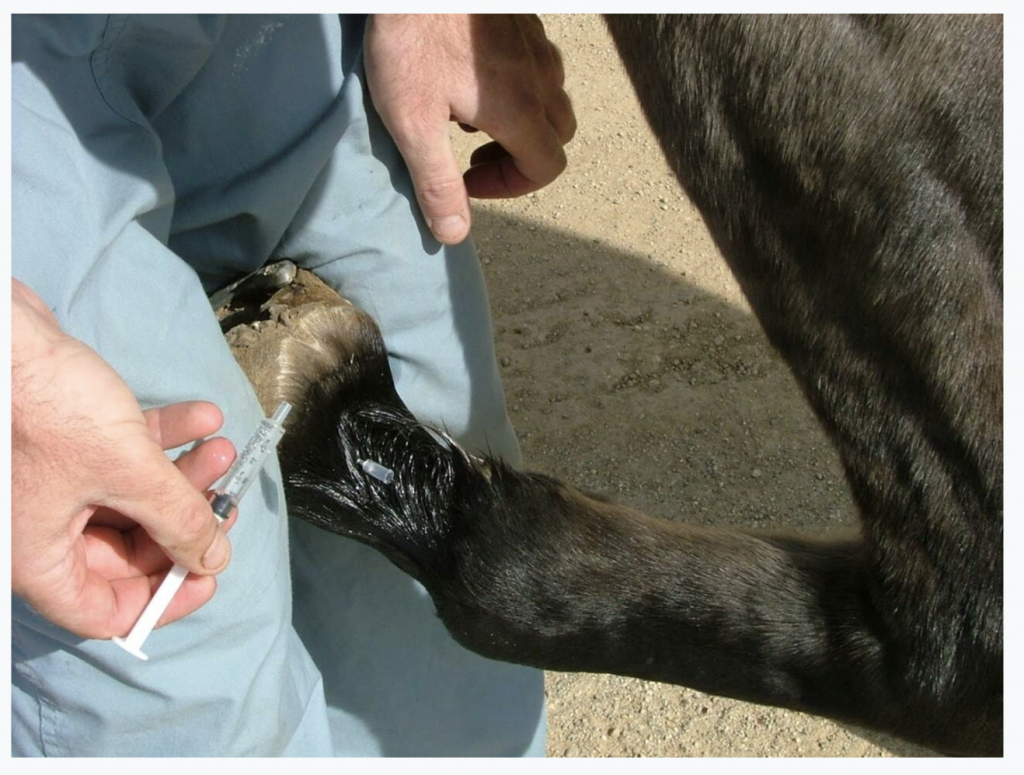
A vet in our practice performs a Palmar Digital Nerve Block. This is a vital part of the diagnosis of Navicular Syndrome. Image Courtesy of Thal Equine LLC.
Five minutes after local anesthetic is injected around the PDNs, that region and all the structures within it are numb, and the horse is trotted again. If the pain has been originating from structures from within this “blocked” area, the lameness is now improved. If pain has been coming from somewhere higher up the limb, the horse is still lame, heel lameness would be ruled out, and subsequent higher blocks would need to be performed to determine the origin of the pain.
In most navicular horses, once one foot is blocked, then lameness in the opposite forelimb becomes more obvious. That foot too can be blocked similarly, At this point, the horse should be moving without lameness.
So now we know that the horse has pain in the rear of the hoof, how can we determine the particular structures involved? Remember…. we did not just block the navicular bone. Within the numb region are sensitive tissues of the hoof capsule, digital cushion, frog, sole, navicular bone, bursa, multiple supporting ligaments, DDFT, part of the coffin bone, part of coffin joint, etc. It is complex!
In some cases, additional information can be gotten from performing a direct coffin joint or navicular bursa block.
IMAGING TO UNDERSTAND THE DETAILS OF THE CONDITION
If the exam and nerve blocks define the back half of the hoof as the painful area, then a series of high quality digital radiographs (x-rays) of the area are taken to visualize the bones of that region. Sometimes the radiographs show obvious navicular changes, which help confirm the diagnosis, but other times the bone appears normal radiographically. Horses with severe bony changes in radiographs tend to have more advanced disease and are often more difficult to treat.
A side (lateral) view of the lower limb is very important to assess hoof/pastern angle and shoeing. This one shows that the shoe is placed further forward than might be ideal.
A side (lateral) view of a limb with a severely “broken back dorsal hoof wall/pastern angle”. Ideally, these two lines should be parallel.
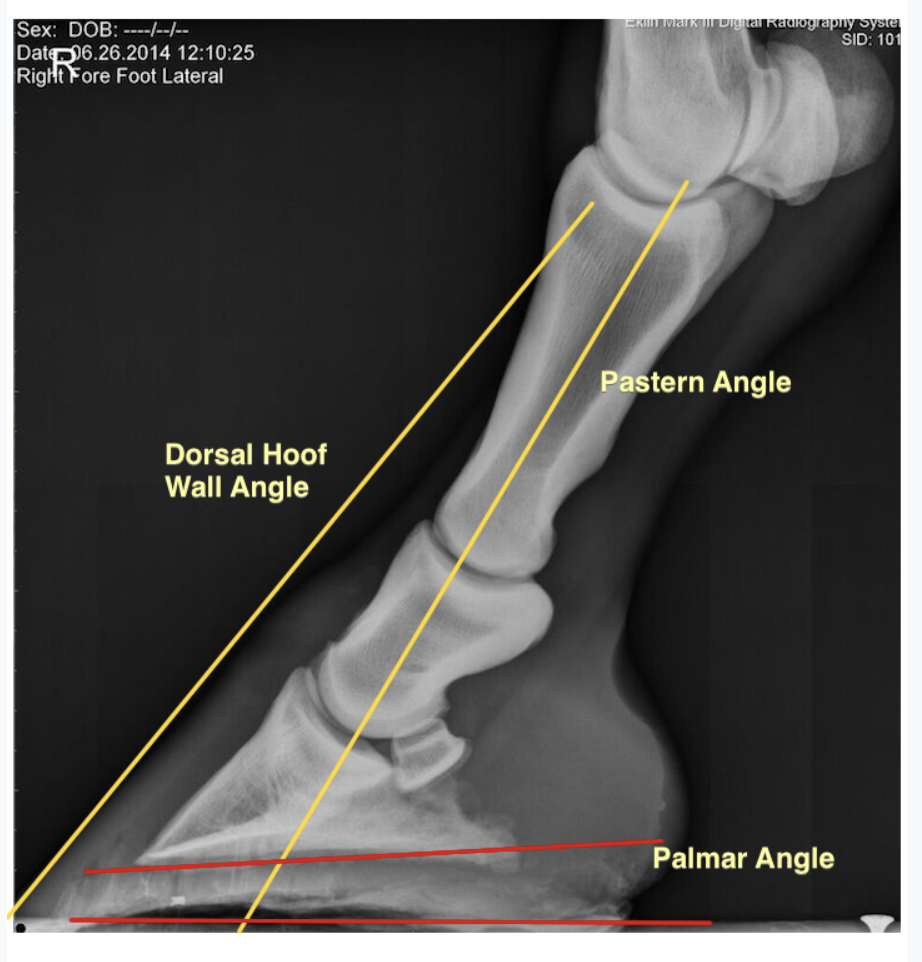
In contrast, a side (lateral) view of a limb showing ideal alignment of dorsal hoof wall and pastern angles.
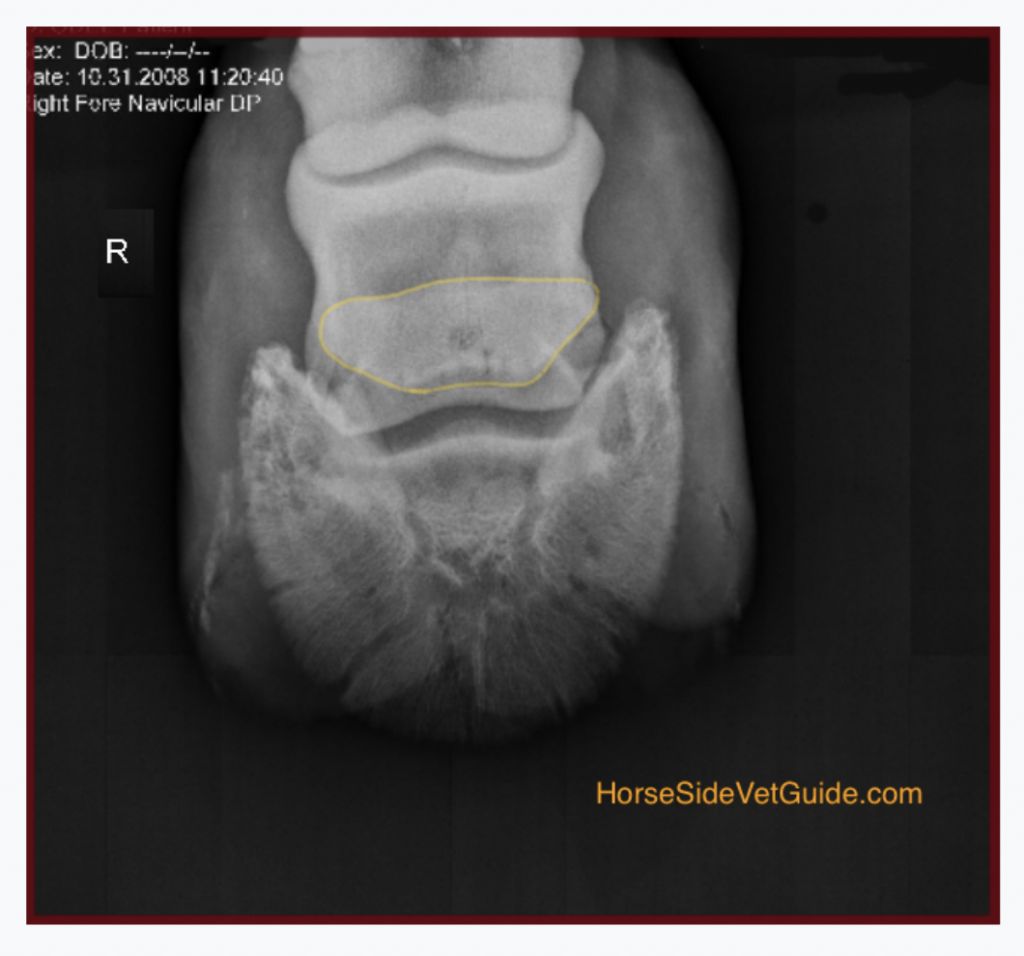
A view of an abnormal navicular bone from above. The navicular bone is outlined in yellow and shows a dark “hole” in the center, which corresponds to an area of bone loss within the navicular.

The Navicular Skyline radiograph taken looking down between the heels. This is an appearance of a normal bone.
Ultrasound, which is so useful for imaging other soft tissues, is not very helpful in these cases because of its inability to penetrate the hoof. In some cases, however, limited additional information can be used by ultrasounding through the well-trimmed, softened frog.
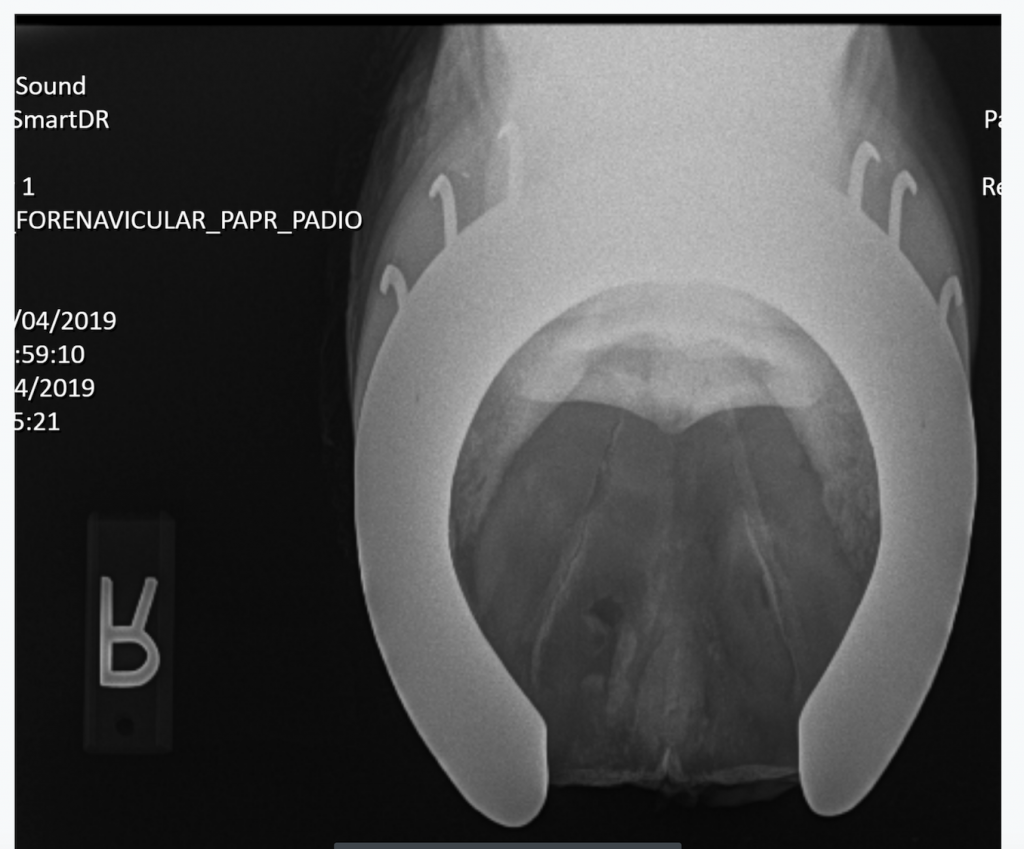
An example of a navicular skyline radiograph in which there is an erosion through the rear part of the bone, a bad abnormality to find, and a tough case to treat. In contrast to prior normal reference image.
In cases where the horse blocks to the heel, but there is no x-ray change, we assume that soft tissue – supporting ligaments, tendons, bursa, digital cushion, etc. – must be the primary contributors to the pain, or that the bone does actually hurt, but that early or mild changes in the navicular bone might simply not be visible via radiography.
MRI: Shining a Light on a Whole Host of Problems We Only Guessed Existed
Only MRI (Magnetic Resonance Imaging) allows visualization of both soft tissue and bone of the lower limb in clear detail, allowing us to see the wide variety of soft tissue and bone disease that can make up Navicular Syndrome and other more subtle conditions of this part of the foot. Unfortunately, MRI is still not widely available, often requires general anesthesia, and is costly. Therefore, in many cases, the diagnosis is made and treatments will be attempted without the benefit of MRI. A variety of other diagnostic tools – CT scan, Nuclear Medicine – can add information but are less important than those discussed.

An MRI “slice” taken through the center of the lower limb. Only MRI shows both soft tissue and bone in such fine and accurate detail. The navicular and deep digital flexor tendon are very obvious and detailed.
YOUR VET’S ROLE: TREATMENT & MANAGEMENT
Once a horse is diagnosed, treatment and management can be considered. Many horses diagnosed with navicular syndrome can be helped with treatment, but there is no silver bullet – no one-time treatment – to “cure” the condition. Rather, most horses with navicular syndrome are managed over time, using a mix of individualized medical treatments, farriery, and work and exercise recommendations. There are a few key general points of treatment:
.
- • The more quickly Navicular Syndrome is diagnosed and treated, the better the chance for success.
- • Horses with conformational defects are at a mechanical disadvantage – heavy horses with tiny feet often cannot be made sound, no matter the treatment.
- • An important part of treatment is that riders/owners/trainers adjust expectations to accommodate the horse’s reduced ability to work, and understand that management might always need to be considered.
REST- We almost always recommend a variable length break from intense work like galloping or jumping. That doesn’t mean strict stall rest. As mentioned before, many horses with navicular syndrome seem to do best kept in light to moderate daily exercise.
FARRIERY: A CORNERSTONE OF TREATMENT
Consistently scheduled and proper trimming and shoeing is a key component of managing this condition. A horse diagnosed with navicular syndrome needs to start with a “correct trim”. Shoeing then allows additional mechanical manipulation that can further help mechanics. Radiographs provide vital information to guide the shoeing.
The mechanics of the hoof that are important to consider include the movement of the center of articulation over the center of the hoof, aligning the hoof-pastern axis, extending the heels to the base of the frog if possible, and shortening the breakover.
A side (lateral) view of the lower limb is very important to assess hoof/pastern angle and shoeing. This view shows that the shoe is placed further forward than might be ideal.
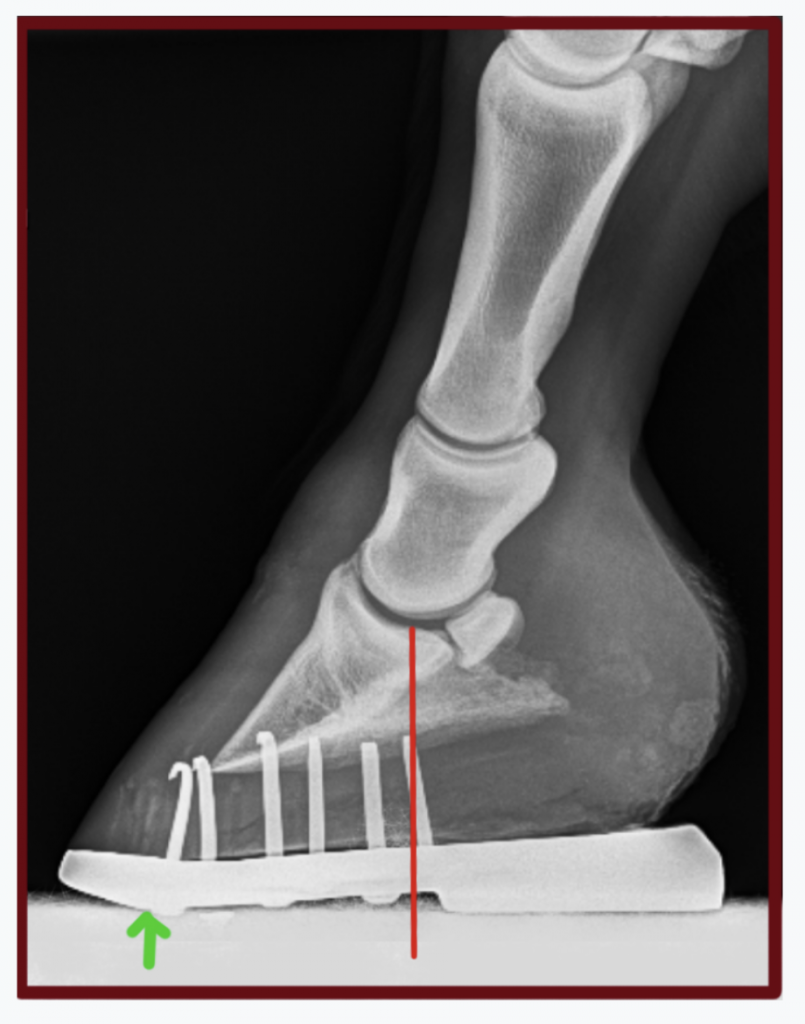
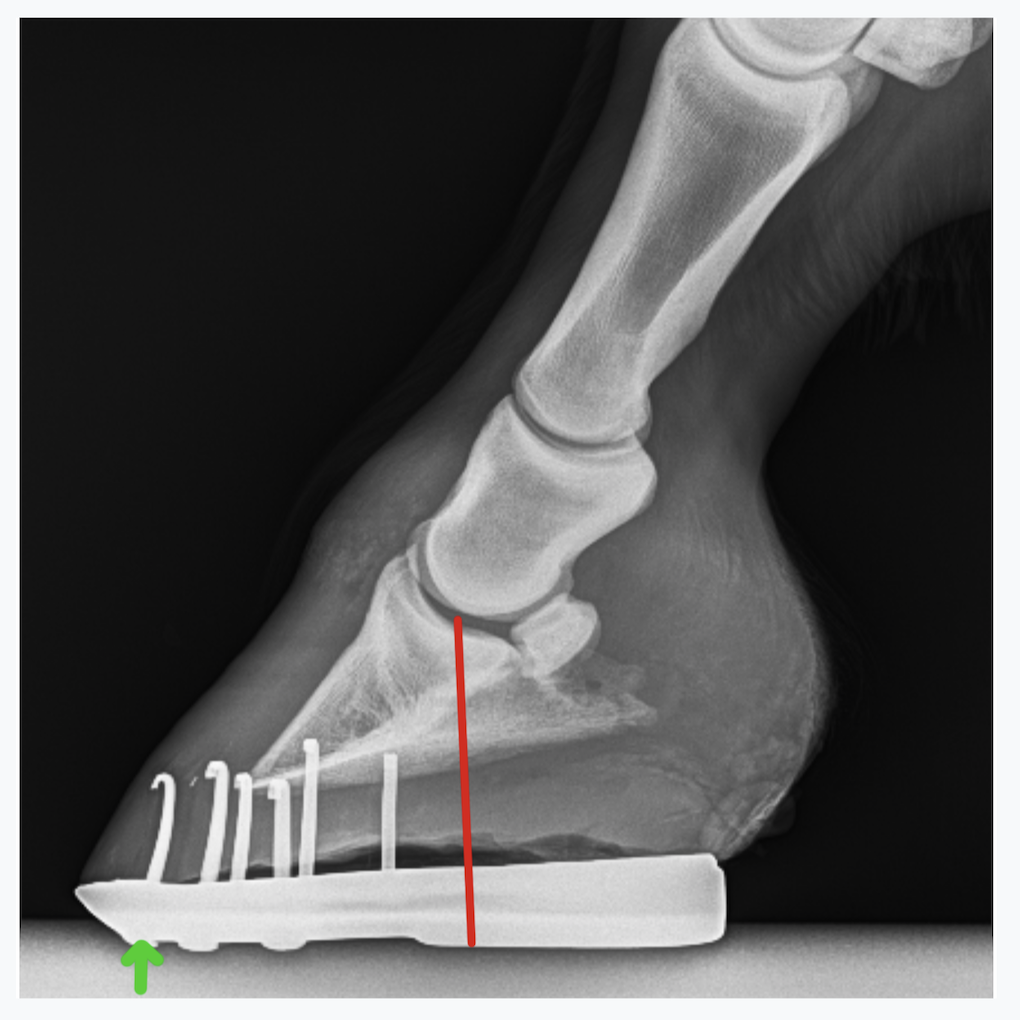
Here, a similar shoe with more wedge, improved center of rotation and breakover moved back further. Red line- center of rotation of the coffin joint, green arrow – breakover.

Radiograph showing mechanics of the roller motion shoe on the hoof, one way to address navicular syndrome. The red line is the center of rotation of the coffin joint. The idea is to relieve stress on the heel and navicular apparatus and thus relieve pain, and to protect the area from direct trauma.

The roller motion shoe has just been made from steel bar-stock. It is upside down, but you can see the mechanics. Toe is to the left.

The roller motion bar shoe on the sole of the hoof.
There are many different shoe designs, with the main intent being to wedge the horse to the normal axis, and in soft footing, to reduce overextension of the coffin joint, which could add load to the navicular. A bar shoe is commonly used to “protect” the heel by decreasing the heel’s sinking into the ground.
There is lots of disagreement in the profession about the way to manage these horses’ feet. Some advocate removing shoes altogether and managing barefoot. Different farriers will attempt to achieve the mechanical objectives using different materials and techniques.
What is important is that basic principles are followed – and most importantly – that whatever is done results in the horse being more comfortable and better able to do their job. Working with an experienced veterinarian and experienced farrier gives the horse the best chance of soundness.
VETERINARY TREATMENT
In the past, all we really knew about this condition was that there was degeneration of the navicular bone. We could see this happening via x-ray changes in some affected horses. The idea was that if this could somehow be stopped, then pain coming from the area would stop and the horse would be more comfortable. In many horse, there turns out to be truth to this.
Many of us inject medication (usually steroids) into the coffin joint and/ or navicular bursa in order to break the cycle of pain and inflammation in the foot. There is usually some improvement in lameness grade following these injections. Often it can hard to tell just how much they help, because we often couple injection with changes in shoeing. If improvement is significant and lasts for months, it is repeated. In some cases though, improvement is only transient and other strategies need to be considered.
Systemic medications (oral or injectable medications) are often part of the treatment plan. A wide assortment of medications have historically been used to treat this syndrome. When I started practice in the early 1990s, the most commonly used drug was isoxsuprine, a vessel-opening drug (vasodilator) that supposedly encouraged increased blood supply to the bone. Although some horses do improve while on this drug, it was found that it in fact did not increase blood supply to the foot. We really don’t know for sure why isoxsuprine helps in some cases.
These days, a commonly-used drug class is the bisphosphonate class (Osphos and Tildren). Bone is a very dynamic tissue, constantly being laid down and resorbed (taken up). Bisphosphonates work by stopping bone resorption. It makes sense that these might be useful, given that a visible part of Navicular Syndrome appears to be breakdown of the Navicular Bone itself. As we know though, the disease process is often more complex than that. Some horses with heel pain do respond to these drugs but some don’t. They should only be used under vet supervision, and per the label dosage and interval. If they don’t seem helpful, other approaches will need to be used instead.
Phenylbutazone (bute), firocoxib, and other NSAIDS control pain and inflammation and decrease lameness, but because of side-effects, are often not a good answer for long-term maintenance. Firocoxib is a safer, but weaker alternative than bute for long-term blunting of pain and inflammation in these horses. Typically, as the disease progresses, NSAIDS have decreasing effect.
Although widely used, like PSGAG (Adequan) and Sodium hyaluronate (Legend) and oral joint supplements are not thought to provide much benefit for horses with navicular syndrome.
Extracorporeal Shockwave can be helpful in some cases, particularly those that involve the rear part of the bone (flexor cortex). I have had some very positive results using this therapy in a handful of cases that did not respond to other treatment.
A variety of surgical procedures (like cutting of the navicular suspensory ligaments) can change the mechanics of the navicular and can be helpful in some cases, but are case specific and are not reliable.
For cases that don’t respond to treatment, MRI might be necessary to further define the injury, not only to the navicular bone, but also potentially to the supporting ligaments, the bursa, the coffin joint, and/or the deep digital flexor tendon. The information in an MRI image might in some cases, allow precise, targeted treatment of these individual structures. With the information from an MRI, perhaps a tiny tear in the deep flexor tendon could be “cleaned up” arthroscopically, or stem cells might be injected into it. Long-term rest might also be vital in allowing that injury to heal, whereas it wouldn’t be expected to help the horse with more typical bone degeneration. Similarly, the horse with the tendon tear would be unlikely to have a positive response to a bisphosphonate drug.
For horses with advanced disease that cannot be made comfortable any other way, Palmar Digital Neurectomy (nerving) can be helpful as a last alternative. This procedure involves removal of a segment of each of the heel (palmar digital) nerves in the back of the pastern. This provides long-term relief of pain through numbing of the area, but obviously does not correct the condition causing pain. The cycle of destruction in the hoof usually goes on, and in some cases may accelerate owing to more loading of the limb.
Neurectomy has important potential side effects to consider. In cases with a damaged deep digital flexor tendon, ongoing degeneration of that structure through increased wear may eventually cause rupture, requiring euthanasia. Nerve regrowth is common after a few years, with return of pain and lameness. A horse with no sensation in the sole of the hoof may step on a nail and not show lameness, allowing the damage to worsen. These and other disadvantages aside, neurectomy can be a helpful salvage procedure for some horses, prolonging a quality life in a situation that would otherwise require euthanasia.
YOUR ROLE
As an equine caretaker, your role is just as vital as the experienced vet’s or farrier’s role:
.
- • Be on the lookout for this condition, especially in the predisposed breeds, and especially when you are considering buying a horse.
- • Know the basic mechanics and anatomy of the horse’s foot. Know what it should look like and recognize major deviations in a horse’s hoof capsule.
- • Get your vet involved early if you suspect lameness.
- • Once a horse is diagnosed, you will need to administer the treatment and management as prescribed.
- • You will also need to objectively monitor the horse’s response and communicate your observations to your vet.
CONCLUSION
Navicular Syndrome is a very common but complex condition. A complete diagnosis requires a thorough diagnostic approach. Your vet should be very familiar with the many faces of this syndrome, be confident with diagnosis, and know the treatment options. If they are not, they should be willing to refer you to someone who is. The vet MUST work with an experienced farrier to implement the necessary farriery changes. It is the team approach that results in success in this and other conditions of the foot. Whether or not MRI can be a part of diagnosis depends on the particular case and your resources.
I hope this article is of value to you – Doug Thal DVM Dipl. ABVP
REFERENCES
Baxter G. Manual of Equine Lameness: Wiley Blackwell 2006 pp. 225-229
Floyd A. Mansmann R. Equine Podiatry. Saunders 2007
O’Grady S. Strategies for shoeing the horse with palmar foot pain: www.equipodiatry.com/article_palmar_pain

















{kind=link}
Thank for share your logical article.
Heel pain is very common in horses with navicular syndrome. This may be due to strain and inflammation of the ligaments supporting the navicular bone, reduced blood flow and increased pressure within the hoof, damage to the navicular bursa or DDF tendon, or from cartilage erosion.
Thank you for the best, most logical and comprehensive summary I have read of this devastating disease.
I would encourage anyone dealing with this question to seek out an MRI and get answers. It provides so much more information and has helped us make humane and caring decisions.